"Buy ropinirole with american express, symptoms quitting tobacco".
By: M. Irmak, M.B.A., M.D.
Clinical Director, Ponce School of Medicine
Over a period of 24 weeks antiretroviral-naive subjects received a combination of zidovudine 48 Astragalus A Astragalus + Food No interactions found treatment 5 shaving lotion purchase 1mg ropinirole visa. Use and indications Avens has been used as an astringent in diarrhoea symptoms for pregnancy discount ropinirole 1 mg with visa, a haemostatic and an anti-inflammatory medications causing hair loss purchase ropinirole 2mg otc. Constituents the main actives found in the whole plant are the tannins medicine x stanford discount ropinirole 2mg with visa, gallotannins and ellagitannins, including sanguiin H6, casuarictin, pedunculagin, potentillin and tellimagrandin. Other polyphenols include gallic, caffeic and chlorogenic acids, gein (a phenolic glycoside of eugenol), flavonoids and volatile oil containing eugenol. The bacosides have been found, in a number of studies, to enhance the memory and cognitive processes. Bacopa has also been used as an anti-inflammatory, analgesic, antipyretic, sedative, and for the treatment of asthma and bronchitis. Recent toxicological studies suggest that the herb is relatively safe in normal use. Constituents Bacopa contains a wide range of triterpene glycosides, including the bacopa saponins, known as bacosides and bacopasaponins. Cucurbitacins, known as bacobitacins and cucurbitacin E, the alkaloids brahmine and herpestine, phenylethanoid glycosides (including the monnierasides and plantioside B), and the flavonoids apigenin and luteolin have also been isolated. For information on the pharmacokinetics of individual flavonoids present in bacopa, see under flavonoids, page 186. For information on the interactions of individual flavonoids present in bacopa, see under flavonoids, page 186. Use and indications Bacopa is an important herb in Ayurvedic medicine, which is 50 Baical skullcap Scutellaria baicalensis Georgi (Lamiaceae) B Synonym(s) and related species Huang qin. Pharmacokinetics No relevant pharmacokinetic data found specifically for baical skullcap, but see flavonoids, page 186, for information on individual flavonoids present in baical skullcap. Interactions overview Baical skullcap is the constituent of a number of Chinese medicines, such as sho-saiko-to, saiko-ka-ryukotsu-borei-to and sairei-to; these interactions are covered under bupleurum, page 89. For information on the interactions of individual flavonoids present in the herb, see under flavonoids, page 186, particularly the monograph Flavonoids + Ciclosporin, page 190, where baical skullcap was given as a source of flavonoids. Use and indications Baical skullcap root has been used traditionally, especially in Chinese medicine, as a remedy for inflammation, infections, dermatitis, allergic diseases, hyperlipidaemia, atherosclerosis and stress-related disorders. B Baical skullcap + Carbamazepine For mention that saiko-ka-ryukotsu-borei-to and sho-saiko-to (of which baical skullcap is one of a number of constituents) do not affect the pharmacokinetics of carbamazepine in animal studies, see Bupleurum + Carbamazepine, page 90. Baical skullcap + Ofloxacin For mention that sairei-to and sho-saiko-to (of which baical skullcap is one of a number of constituents) do not affect the pharmacokinetics of ofloxacin, see Bupleurum + Ofloxacin, page 90. Baical skullcap + Ciclosporin For mention that baical skullcap, given as a specific source of flavonoids, may affect the pharmacokinetics of ciclosporin, see Flavonoids + Ciclosporin, page 190. For conflicting evidence from animal studies that sho-saiko-to (of which baical skullcap is one of 7 constituents) might increase or decrease the rate of absorption of tolbutamide, see Bupleurum + Tolbutamide, page 90. Balm of Gilead Populus6gileadensis Rouleau and other Populus species (Salicaceae) B Synonym(s) and related species Balsam Poplar, Gileadensis, Poplar buds. Use and indications Balm of Gilead has expectorant, stimulant, antipyretic and analgesic activity, and is used mainly in cough mixtures. Pharmacokinetics No relevant pharmacokinetic data found for Balm of Gilead, but note that salicin, a constituent of Balm of Gilead, is metabolised to salicylic acid in the body. See also flavonoids, page 186 for information on the flavonoid components of Balm of Gilead. Interactions overview Constituents the leaf buds, collected before they open, contain phenolic glycosides including salicin (a salicylate) and populin, and a volatile oil consisting of -caryophyllene as the major component with cineole, bisabolene, farnesene and actophenone. Flavonoids present include apigenin, chrysin and others, and some Populus species may have constituents that differ slightly. Balm of Gilead contains salicin, a precursor of salicylic acid, and clinically relevant levels of this have been achieved by taking some herbs, although this does not necessarily equate to the antiplatelet effect of the herb. For a discussion about the use of herbs with antiplatelet effects in conjunction with antiplatelet drugs and anticoagulants, see willow, page 399. See also flavonoids, page 186 for information on the interactions of individual flavonoid components of Balm of Gilead. Use and indications Bayberry bark is used for coughs and colds, and for diarrhoea and other gastrointestinal disorders. Constituents the root bark, which is used therapeutically, contains triterpenes including myriceric acid A, myrica acid, myricadiol, myriceron caffeoyl ester, taraxerol and taraxerone, and the flavonoid, myricitrin.
T4 makes up 90% of the hormone secreted by the thyroid; the remaining portion is T3 medicine 101 order cheap ropinirole line. Most T3 and T4 is bound to serum proteins; only about 1% is unbound and free to enter cells to carry out thyroid functions symptoms 4dp5dt fet purchase ropinirole without a prescription. This article reviews the pathophysiology of hypothyroidism medications you can take while pregnant for cold generic 2mg ropinirole amex, as well as its causes medicine mart purchase discount ropinirole line, symptoms, diagnosis, treatment, and nursing care. Secondary hypothyroidism is caused by pituitary gland dysfunction, and tertiary hypothyroidism results from problems with the hypothalamus. Other autoimmune diseases, such as scleroderma or amyloidosis, can cause hypothyroidism A rare outcome of hypothyroidism is myxedema coma, which is severe physiologic decompensation that can lead to death. Myxedema coma is a true medical emergency with a high mortality rate, but with iodized salt and improved medical surveillance, the annual incidence is only 0. Because the turnover of new cells is delayed with slowed metabolism, her skin has a characteristic dry, rough quality. People with hypothyroidism experience a slowing of metabolic processes, which can result in fatigue, slow speech, constipation, cold intolerance, weight gain, bradycardia, and decreased deep tendon reflexes. One study showed the most common symptoms are tiredness, dry skin, and shortness of breath. The signs of hypothyroidism are numerous, often subtle, and not specific to hypothyroidism. Measuring thyroid hormone levels in the blood is the only way to make a definitive diagnosis. Because symptoms overlap with so many other conditions, diagnosing hypothyroidism based on clinical presentation alone is not possible; laboratory testing is required. Fortunately, we can measure thyroid hormone levels in the blood and pinpoint a diagnosis. This schedule change may be particularly helpful for patients who take many medications in the morning that are incompatible with levothyroxine. Prognosis Nursing considerations Teach patients about the many drug interactions with levothyroxine and about the importance of establishing a daily routine to help maintain even hormone levels. Levothyroxine should be taken on an empty stomach with water, at least 1 hour before eating. And levothyroxine is incompatible with many other medications, so it should be taken alone. Medications that bind with levothyroxine and reduce its bioavailability include bile acid sequestrants (such as sevelamer), calcium supplements (including calcium acetate, carbonate, and citrate), aluminum, magnesium, lanthanum, and simethicone. Taking levothyroxine with anticoagulants can increase the effect of anticoagulants. With some medications, such as antacids, advise patients to allow 4 to 6 hours to pass between taking each medication. Although patients are traditionally instructed to take levothyroxine first thing in the morning on an empty stomach, a randomized double-blind study showed that taking After beginning levothyroxine, symptom improvement can take up to 6 weeks, and dosing may need to be titrated, which is usually done at 3to 6-week intervals. Patients should begin to feel a restored sense of energy, improved cognitive function, thickening of hair, and other symptom improvements. Your astute call enabled her to get the treatment she needed to improve her quality of life. Treatment Hypothyroidism is treated with synthetic T4 (levothyroxine), which is available in tablet, soft gel, and liquid form, although tablet is the most common. Studies show no benefit to taking both T4 and T3, 46 American Nurse Today Dorothy Moore is a staff nurse at Kaiser Permanente Emergency Department, in Oakland, California, and an adjunct lecturer at California State University in Hayward. This guideline document reviews the risks and benefits of treating subclinical hypothyroidism in female patients with a history of infertility and miscarriage, as well as obstetrical and neonatal outcomes in this population. Studies were eligible if they met one of the following criteria: primary evidence (clinical trials), that assessed the effectiveness of a procedure correlated with outcome measure (pregnancy, implantation, or live-birth rates), meta-analyses, and relevant articles from bibliographies of identified articles. The quality of the evidence was evaluated using the following grading system and is assigned for each reference in the bibliography: Level I: Evidence obtained from at least one properly designed randomized, controlled trial. Dramatic results in uncontrolled trials might also be regarded as this type of evidence. The strength of the evidence was evaluated as follows: Level A: There is good evidence to support the recommendations, either for or against.
Generic 1 mg ropinirole with amex. Awards highlights 2008 - part 1 of 2.
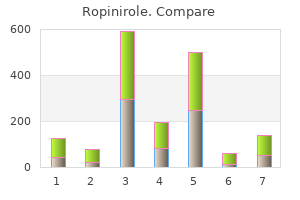
However symptoms of ebola discount ropinirole 0.5mg on-line, the real existence of this condition is debated and specific markers are lacking treatment concussion buy 0.5 mg ropinirole with visa. There are more and more patients like Patty and the obesity epidemic continues without a plateau in sight medicine 74 cheap ropinirole 1 mg without prescription. Body weight change in kilograms Fat-free mass change in kilograms Fat mass change in kilograms What happened at 6 years? Mechanism: stimulant similar to amphetamine Side effects: dry mouth insomnia dizzyness hypertension tachycardia abuse potential About 50% drop out of therapy from side effects medications via g-tube buy ropinirole 0.5 mg on line. Europe approved, then later withdrew because of suicides (2x risk of psychiatric disorder and 10% depression, 1% suicidal ideation Qsymia the Good. Travel to Myanmar to uncover the elusive source of his fevers 65-year-old man returned from Myanmar, p/w 2d fevers and a rash. Framing the error of initiating diagnostic reasoning by overvaluing an item of clinical information that is presented early in the process. Anchoring the formulation of an initial probability of a diagnosis based on information at hand, and not adjusting this probability as new clinical data are obtained. Review of differences in the screening guidelines and reconciling theses differences. Review of available tools in addition to guidelines to risk stratify your patients. There is at least moderate certainty that net benefit is small Recommends against the service. There is moderate to high certainly that service has no benefit or that harms outweigh the benefit Current evidence is insufficient to assess benefits and harms of the service. Estimated incidence in 2018; 266,120 Estimated deaths in 2018; 40,920 5 year survival; 89. How frequent: every year or every 2 years Who should be considered for earlier screening. Women with family history, parent, sibling or child with breast cancer are at higher risk and may benefit from starting screening in their 40s. This was not addressed again in 2016 as digital mammography is now widely available. Grade D I I Breast Cancer Screening: American Cancer Society Population 45-54 55 and older 40-44 years Recommendation Mammography annually Biennial mammography Women should have the opportunity to begin screening at 40-44 years Should have the opportunity for screening as long as their overall health is good and life expectancy of 10 years. Non Hispanic White and non Hispanic Black women have the highest risk of breast cancer and their risk of breast cancer is now similar. Personalized arm will be assessed for breast cancer risk and given a genetic test. All women should have a risk assessment with family history and risk factors in to account no later than 30 years of age. There is very little data on racial and ethnic minorities and this should be considered in decision making. For age 30 and older recommendation as above or if the cotest is negative can be screened every 3 years. Current draft recommendations are for individualizing the decision for man 55-69 years with grade C and recommends against screening in man older than 70 years of age. This included African American men and men who have a first degree relative diagnosed with prostate cancer at an early age( Younger than 65). Age 40 for men at even higher risk ( Those with more than one first degree relative who had prostate cancer at early age). Can be done with single specimen More false positives leading to more colonoscopies and more associated adverse events No bowel prep, anaesthesia, transportation required Insufficient evidence of longitudinal follow up after negative colonoscopy. Keep patient considerations in mind when choosing a screening tests for colon cancer.
Elkins and Administrative Finality In Elkins medicine 6mp medication purchase ropinirole 0.25 mg line, the Federal Circuit provided guidance as to the applicable jurisdictional finality standard in the context of appeals from decisions that do not dispose of all claims but instead include a remand symptoms questionnaire ropinirole 1 mg otc. Elkins established that judicial review is available for a claim for which final judgment has been entered even if other claims presented in the same appeal have been remanded medicine youth lyrics purchase ropinirole 2 mg with mastercard. The Federal Circuit explained that in deciding that it could treat the claims as separable on appeal medications parkinsons disease buy ropinirole 0.25mg free shipping, it was adopting the approach in Dewey Electronics Corp. Applying this Elkins standard to an appeal from our Court, the Federal Circuit concluded that, because the legal issues presented on appeal were all distinct (i. Court of Appeals for Veterans Claims has jurisdiction to review a decision concerning one of the issues that comprise a claim, i. The Federal Circuit further stated: "Rather, we have recognized that the unique statutory process of adjudication through which veterans seek benefits may necessarily require that the different issues or claims of a case be resolved at different times, both by the agency of original jurisdiction and on appeal. In meritorious cases where the Board denies benefits based on a particular issue with distinct criteria and remands for further adjudication another issue of establishing entitlement to benefits, a veteran might otherwise have to wait years for resolution and possibly benefits to which he or she is entitled. Unlike the factual circumstances presented in Bingham, however, where the Board denied a claim for service connection on one theory and was silent as to other theories of service connection, in the present case, the Board specifically remanded a separate theory for development, thereby foreclosing any argument that its denial of direct service connection could be interpreted as a final decision on the separate theory of presumptive service connection. It is unlikely that the Board will spend its resources adjudicating the first matter if that were the law, and the Board might very well decide that it would be more efficient to delay any adjudication until all claims for benefits, or theories in support of a claim for benefits, were ready for a decision. The veteran would thus be denied the opportunity of judicial review of an adverse decision until all issues addressed in the Board decision or all possible bases for supporting a claim for benefits have been finally decided. This, in turn, could render any review by this Court of the decision on the anxiety neurosis claim meaningless and a waste of judicial resources. Accordingly, the Court determined that piecemeal review could render a decision on one claim "meaningless" and would be a "waste of judicial resources. Because the claims appeared "so closely tied" together, the Court concluded that the Board decision did not constitute a final decision and dismissed the appeal for lack of jurisdiction. The Court today overrules Harris to the extent it stands for the proposition that this Court has no jurisdiction over a Board decision that denied a claim if that claim is "inextricably intertwined" with another claim that the Board remanded. The Court has jurisdiction over such matters on direct appeal, but may decline to exercise its jurisdiction in such cases, as we frequently do. Overruling Harris, we now hold that where a Board decision purports to be a final decision, the Board issues a notice of appellate rights, and the appellant timely appeals to the Court, this Court has jurisdiction to review the Board decision for error. We hold that only after the Court determines that it has jurisdiction does it then engage in consideration of questions concerning whether the appeal involves multiple claims or issues that are inextricably intertwined. Even if this Court were to hold that there are two claims involved here, Harris dictates that we determine, as part of this appeal, whether the "claim" for service connection for a lung condition on a direct basis that was denied in 1998 is "inextricably intertwined" with the "claim" for presumptive service connection for a chronic disability resulting from an undiagnosed illness based on service in the Persian Gulf. If so, Harris would not have permitted this Court to have jurisdiction over an appeal filed within 120 days of the 1998 denial but would permit jurisdiction now to review the 1998 denial as part of the current appeal of the denial of service connection under the presumptive provisions for Persian Gulf W ar veterans. In such a case, the Court can then determine whether the benefits denied or limited are inextricably intertwined with a remanded issue or claim, or whether the Board erred in issuing the denial or limitation of benefits that was appealed. Parties are well-served by a process that allows the Court to review assertedly final decisions to determine (1) whether one issue on which the Board denied benefits is inextricably intertwined with other issues that the Board remanded, and (2) whether such a Board decision should be reversed, modified, or the matter remanded, based on Board error, including misapplication of the law, failure to develop a complete record, or other defects that would otherwise not be addressed for years thereafter. Claimants not satisfied with a clear, final decision of the Board, accompanied by notice of their appellate rights, should appeal any such decision in a timely manner (or request Board reconsideration) to preserve those appellate rights. A claimant should understand that "Board denial" on the issues coupled with a notice of appellate rights means "file an appeal or the denial becomes final," because it is in the control of the claimant, not the Court or the Secretary, whether to appeal once the Board issues its decision. If an appeal is filed, the Court will determine issues of finality and whether the issues or claims are inextricably intertwined on a case-by-case basis. Failure of a claimant to appeal (or seek reconsideration) presents the risk, as we see in the case before us, that the matters finally decided by the Board will not be appealable after the time to appeal passes. First, the Board denied benefits based on entitlement to service connection on a direct basis. Second, the Board remanded, for further development, entitlement to service connection under 38 U.